

(ZENIT News / Washington, 12.18.2025).- For decades, public discussion about abortion and women’s mental health has tended to focus on the immediate aftermath of the decision. Relief, distress, or a mixture of both were generally assumed to be short-lived, resolving within months or a few years at most. A new peer-reviewed study now challenges that assumption in a way that is difficult to ignore: for a substantial proportion of women, the emotional impact of pregnancy loss — including abortion — does not recede with time, but endures for decades.
The research, published in mid-December, draws on a nationally representative sample of American women aged roughly between their early forties and early fifties. Rather than surveying women who were already engaged with abortion providers or counseling services, the study relied on random sampling, a methodological choice that strengthens the weight of its conclusions. Nearly two thousand women participated, with abortion and miscarriage rates closely mirroring national averages.
One of the study’s most striking findings is that approximately 40 percent of women who experienced a pregnancy loss reported that their most intense negative emotions were still present, on average, twenty years later. This persistence of distress was not limited to any single type of loss, but it was especially pronounced among women whose abortions were experienced as morally conflicting, unwanted, or coerced.
Unlike earlier research that treated abortion as a uniform experience, this study took a more nuanced approach. Women were asked to describe how their abortion aligned with their own values and preferences at the time. Four distinct groups emerged: those who freely desired the abortion, those who accepted it despite an internal conflict with their values, those who did not want it, and those who felt forced into the decision. The emotional outcomes varied dramatically across these categories.
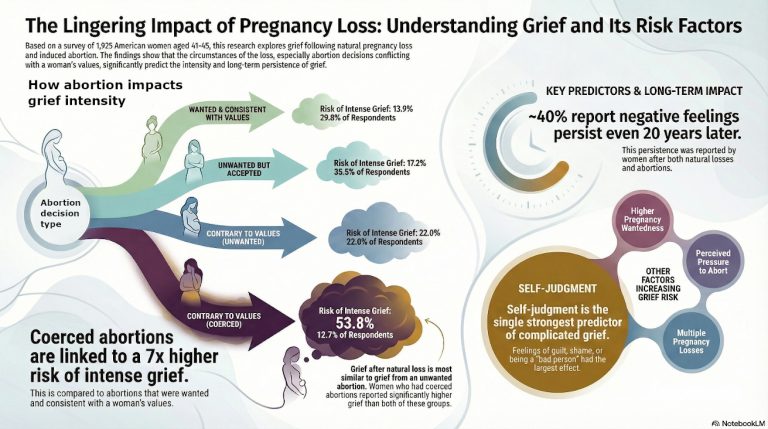
While grief symptoms appeared across all groups, the risk of developing prolonged grief disorder — a clinical condition marked by an inability to move from acute grief to an integrated form of mourning — rose sharply as personal freedom and moral coherence diminished. Women who felt pressured or coerced faced the highest risk, with more than half meeting criteria associated with prolonged or complicated grief. By contrast, women who reported wanting the abortion were significantly less likely to show such symptoms, though they were not immune.
The study also documents a constellation of distressing experiences that resemble post-traumatic stress responses: intrusive thoughts, nightmares, flashbacks, and disruptions to work, relationships, and daily functioning. These patterns echo findings from earlier research, including a September study estimating that as many as seven million American women suffer severe emotional distress following abortion. Notably, researchers found no meaningful difference between women whose abortions occurred recently and those whose abortions took place many years ago — suggesting that, for some, time alone does not heal.
A key factor emerging from the data is silence. Feelings of guilt, shame, or internal conflict often discourage women from disclosing abortion histories, even in therapeutic or spiritual settings. Case studies cited in the research indicate that many women receiving mental health care never mention past abortions unless specifically asked. This dynamic may help explain why abortion-related grief remains underrecognized and undertreated.
These findings directly challenge the conclusions of the widely cited Turnaway Study, which has been used to support the claim that abortion poses little to no long-term risk to women’s mental health. By contrast, the new research suggests that distress can emerge late, intensify over time, or remain dormant for years before resurfacing — a pattern familiar in other forms of trauma.
Beyond the statistical analysis, the study has renewed calls for a broader reevaluation of how abortion is framed within healthcare and public policy. The assumption that abortion is inherently therapeutic for women facing difficult pregnancies is increasingly questioned by data showing that psychological outcomes are highly contingent on coercion, value conflict, and social support. Researchers argue that pre-abortion screening should pay closer attention to women who feel pressured or morally torn, as they face a substantially higher risk of long-term harm.
Mental health professionals, the authors contend, also bear responsibility. Routine clinical practice should include sensitive, nonjudgmental inquiry into all forms of pregnancy loss — including induced abortion — to allow unresolved grief to surface safely, even decades later.
For many women, the story told by this research is not one of sudden revelation, but of long-suppressed experience. The loss, the study suggests, did not end years ago. It simply went unnamed — until now.
Thank you for reading our content. If you would like to receive ZENIT’s daily e-mail news, you can subscribe for free through this link.

Publicaciones relacionadas:
 Revealing finding never before published: the real impact of the abortion pill on women’s health
Revealing finding never before published: the real impact of the abortion pill on women’s health
 UN Committee Challenges Selective Abortion Policies, Sparking Debate on Disability Rights
UN Committee Challenges Selective Abortion Policies, Sparking Debate on Disability Rights
 Legal earthquake in Latin America: Inter-American Court of Human Rights rejects abortion
Legal earthquake in Latin America: Inter-American Court of Human Rights rejects abortion
 Surprising study shows birth projections for 2026: only 8 out of every 100 babies will be born on three continents combined
Surprising study shows birth projections for 2026: only 8 out of every 100 babies will be born on three continents combined